
Births continue to fall in many Wyoming hospitals as lawmakers seek remedies for widening gaps in maternity care across the state.
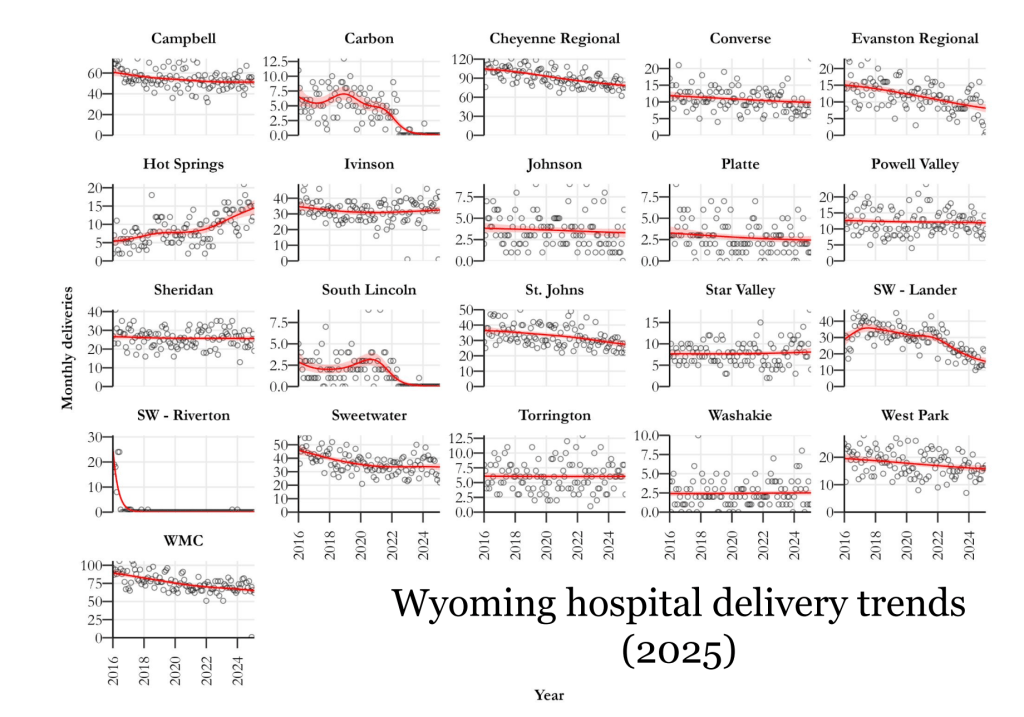
Hospitals in Casper, Cheyenne, Rock Springs, Cody, Douglas and Lander are seeing declining deliveries, data from the Legislative Service Office shows. Four other hospitals — in Riverton, Kemmerer, Rawlins and most recently Evanston — have shut down birthing facilities entirely in recent years. When Evanston announced its closure at the end of 2024, it cited declining demand.
Wyoming’s maternity gap issue appears to be most acute in Central Wyoming, according to Curtis Biggs, Gov. Mark Gordon’s senior policy advisor, where SageWest Hospital in Lander is the main birthing facility serving a huge area of Fremont and Sublette counties.
“We are seeing a concerning trend of a decline in those births in that particular hospital, with a lot of births shifting to Thermopolis,” Biggs told the Legislature’s Joint Labor, Health & Social Services Committee Monday. The latter hospital was the only one presented that has experienced a significant spike in deliveries.
A dearth of maternal health care has made pregnancy and childbirth increasingly tricky in widening swaths of Wyoming, a 2023 WyoFile investigation found. This is evident in Fremont County, where moms are opting to temporarily relocate to places like Denver and even the East Coast to deliver babies. It is evident in Rawlins, where families have to travel Interstate 80, a notorious stretch of highway that closes frequently in the winter months, to deliver in Laramie. And it is evident in Teton County, where overflow patients from elsewhere in the state are straining providers.
Lawmakers made maternity care a top issue of study for the 2024 legislative off-season and began to identify a complicated mix of challenges for providing such care in rural places.
Maternity care is back on the table this summer as policymakers work to improve doctor recruitment, regulations and a complex system of health care reimbursements. Despite some steps forward in the past year, as Biggs explained to lawmakers, the options for families seeking robust maternal health care remain scant or nonexistent in many parts of the state.
The problem
A Wyoming Health Department assessment found that nearly half of the state’s counties lacked a practicing OB-GYN in 2024. The State Scorecard on Women’s Health and Reproductive Care ranked Wyoming 42nd that same year. The state placed behind all of its neighbors.
Solutions have been elusive. Complicating the issue are provider challenges like low birth volume in rural areas, high costs of medical malpractice insurance, financial viability struggles for hospitals, abortion ban impacts on doctors, liability concerns and barriers for midwives to deliver in hospitals.
Health care advocates have called on the state to expand Medicaid, promote midwifery and build partnerships that could boost care.

Along with the 2024 legislative committee study, the OB Subcommittee of Gov. Gordon’s Health Task Force also worked to explore solutions. That group narrowed its focus last summer to three areas: how to better utilize midwives, doulas and family physicians alongside obstetricians in delivery care; the possibility of creating OB medical fellowships to bolster care in Wyoming; and regionalizing the state’s maternity care.
The Joint Labor Committee took up the issue once more as an interim topic in 2025. During its two-day meeting this week in Casper, Deputy Director of the Wyoming Department of Health Franz Fuchs and Gordon’s policy advisor Biggs laid out the situation anew.
“The primary problem we’re really diagnosing this with is hospital viability,” Fuchs said. “We believe that labor and delivery closures are really a symptom of broader financial stress on the hospitals, whether it’s due to low volume generally or management issues.”
That financial stress can come from a host of issues, he said, including low volume of births, management issues, nurse labor shortage and provider recruitment challenges, fewer women of childbearing age creating declining demand and comparatively low Medicaid payment rates. When stressed, hospitals look to offload services, he continued, and labor and delivery is an attractive candidate because it’s not profitable.
Fuchs offered several options for aiding hospitals, including increasing Medicaid hospital payment rates for deliveries, increasing Medicaid payments to delivering providers, increasing funding for provider recruitment programs and increasing provider education opportunities or incentives for medical students.
Other ideas that came up during the meeting were malpractice tort reform, mobile units that can travel to underserved areas and more oversight of the services local hospitals provide.
Steps and directions
Some steps have been taken to address the issue.
Blue Cross Blue Shield of Wyoming is launching a program in July to support maternal health and respond to growing concerns about access to care. The Maternity Care Program will include a subscription service for prenatal vitamins and remote monitoring for high-risk pregnancies or those living in areas with little or no maternity care, among other services.
Another step is a new OB residency track through the University of Wyoming Family Medicine Residency Program at Cheyenne.
“We have residents selected that will be on an OB track starting in July when they start their second year, which means our real goal is for them either then to be able to get into an OB fellowship following residency, or simply to go get a job, hopefully some place in the state,” said Dr. Jacques Beveridge, a Cheyenne OB-GYN.
He also echoed a common sentiment when he urged lawmakers’ “favorable consideration of increasing Medicaid payment.”
As vice president of the Wyoming Hospital Association, Josh Hannes served on the governor’s health task force OB subcommittee.


If the committee is not OK with the current state of maternity care, Hannes said, “and where we believe it’s going to go if there’s no intervention, and you believe that the state has a role to play in doing better, then I think there’s a number of valuable recommendations that have been presented that could take bill form. We would be supportive of those.”
Ultimately, committee members voiced support for pursuing bills that would: help give midwives more authority to deliver; raise Medicaid reimbursements for obstetrics; offer protections for pregnancy resource centers; look into mobile health units; and study other states’ models for helping to pay for malpractice insurance.
In addition, Rep. Rachel Rodriguez-Williams, R-Cody, who chairs the hard-right House Freedom Caucus, said she would like the health department to consider removing the COVID-19 vaccine from the list of recommended vaccines for pregnant women.
Put medical back in hands of doctors. Let them be judge of what patients need. But problem on this is not enough babies being born. The years of abortions have caught up.
Given the dominance of the “Freedom Coalition” in Wyoming, its a wonder there are any women of child bearing age left in the state.
The Freedom Wing-nuts should be proud.
Financial decisions have consequences. Years back I worked as a grant writer in a small rural (at that time public) hospital in Driggs, Idaho, just over the hill from Jackson Wyoming. Our hospital closed down its maternity services because of the federal requirements making it too expensive to staff 24 hours/day for the occasional birth. As a result, a friend of mine had her baby on the top of Teton Pass as she headed to St. John’s in Jackson to deliver. Happy to report that baby has grown into a beautiful young woman but all of us held our breaths that day.
Representative Rachel Rodriquez – Williams and her Freedom Caucus hard right colleagues inserting the legislature into medical decisions: removing Covid -19 vaccinations for pregnant women , barring physicians from using mifiprestone for off label use, endangering women’s health with vague unconstitutional statutes barring abortion all contribute to the abysmal medial care for women in Wyoming. The refusal of the legislature to expand Medicaid has cost lives and contributed to the economic crisis with Wyoming hospitals.
I had my first child a little over seven years ago at Cheyenne Regional. Long story short, I experienced massive postpartum hemorrhaging. The doctors were going to discharge me, but miraculously my child had yet to urinate and we stayed an additional day. I couldn’t walk, couldn’t lift my baby without help, and could hardly think. Thankfully, about 24 hours after baby came, a nurse from Colorado saw my vitals and insisted the doctors look at me. I got two units of blood and the lights in my head turned on again. I still couldn’t walk very well and was very weak for months. Top it off, the billing was horrendous. Depending on the day, we paid too much, too little, charged too much, too little.
I have since tried to visit with OBGYNs here over the years, and every time I come away feeling like they don’t really know what they are doing.
On the other hand, I have had three children in Ft. Collins, the most recent of which I once again had sudden postpartum hemorrhaging, and it was addressed swiftly and professionally. They had the equipment, the people, the calm, the blood, and the knowledge and probably saved my life.
I don’t know what else to say other than all these smaller health groups in Wyoming are just not keeping up with the bigger hospital systems in efficiency, equipment, knowledge of staff, recruitment. And I’m not willing to take on the additional risk on my life and have my babies here. I am so sorry to say it. And I know of at least a dozen other women who have stories similar to mine.
I wish things were different and we had recommendable hospitals in Wyoming, as I was born in Uinta County decades ago, and raised in Park, and my husband was born and raised in Laramie County.
We live im an extremely ligienous society, and the medical p rpvoiders are especily sp becaise pf tjhe fact it is humans health they are especially at risk. I spent my live asa health care provider and finally a Certified Nurse Midwife. The number of things that can go bad during the conception and delivery are tremendous. …..and those having a problem need to blame someone. The health care provider is at the top of the list irregardless of the circumstance. Ending lawsuits for anything except well documented bad care would be a first step.
Medical lawsuits really need to be examined and controlled before we find ourselves totaly without any medical care.
Fremont county expectant moms are voluntarily electing to go to Thermopolis to deliver because they have a brand new L&D unit. Lander L&D unit is ghetto.
Intermountain Health has stepped up in a big way with Uinta Co and surrounding areas following the closure of Evanston’s OB unit. We now have a program called Maternal Health Connection that helps provide prenatal and postpartum care to women and families in the area.
The fake christian war against Women is hurting the state and you’re women family members. Vote them out of office.
I fail to see any religous impact at all on the problem. Health care proividers select where they decide to practice based on many things, I doubt religion has muich impact. I’m a Wyoming native, went to midwifery school in Jackson, MS., went to work for many years providing women’s health care and delivering babies as part of that on the Navajo Res in AZ.
Religion is ALL of the problem. Fake christians telling others what they can do. Doctors do not want to work here.