
Health-care costs and health-care insurance are on people’s minds in Wyoming. In late July, this forum hosted two writers on the pros and cons of Medicaid expansion. Their essays prompted more people to comment — and their comments made it clear that Medicaid expansion is only a piece of the puzzle that is frustrating us in Wyoming, where the numbers say we pay more for health insurance and more for health care than most other folks in the country.
So, here are three people taking a whack at the broader picture. Anne Ladd of Casper, who heads a Wyoming-grown employers’ group working on health care, lays out the case for axing the familiar “fee-for-service” way of paying for health care — and argues that employers and others in Wyoming can take this task on.

Annemarie Albins of Kemmerer, who works in her family’s small business, exposes the costs facing people in Wyoming. She brands health-care and health-insurance costs a crisis, shows its effect on business, and tells politicians to stop posturing and get to work.
And Sandy Shuptrine of Jackson, a former county commissioner who’s worked a bunch of jobs, says we should draw on our compassion to get Medicaid expansion adopted. Lawmakers must understand the majority sentiment favoring the federal program before we collectively tackle causes of high care and insurance costs.
Wyoming’s unique situation means the issues are something we’re just going to have to take on as a state. Wyoming’s a big place but there are not a lot of us — not so many that we can’t figure out and solve common problems. Join this forum, tell your stories and make your proposals. We’ll see whether this discussion will get us somewhere in taking the puzzle apart and defusing the health-care cost crisis.
— Pete Simpson
Employers have to be the change agents in health care
by Anne Ladd
The United States spends about twice what every other developed nation spends on health care whether measured as a percentage of GDP or on a per-capita basis.

Yet, the results of that extraordinary expenditure, as measured by infant mortality, average life span and several other key metrics, put the United States 37th in the world, right behind Dominica and Costa Rica.
We can, and should, do better.
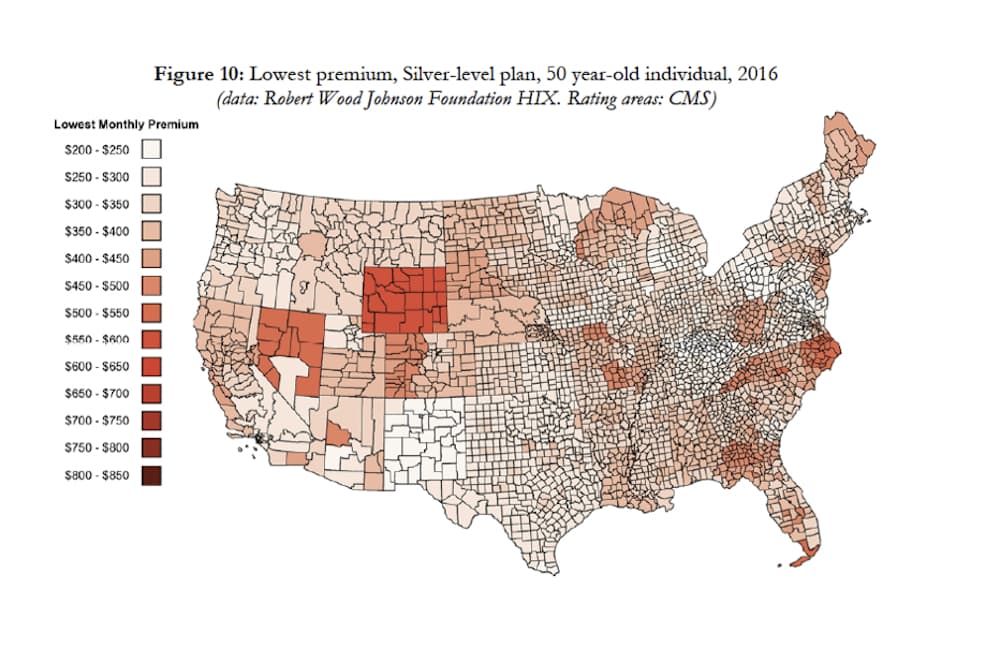
To make matters worse, in Wyoming we pay more for health-care benefits than most other places in the country. That means we get a double whammy when it comes to costs.
The map below illustrates that Wyoming residents face some of the highest premiums in the United States. For example, the lowest-cost Silver-level plan available on the Affordable Care Act Marketplace in 2016 — to an individual non-smoker who is 50 years old — was $586.41 per month in Laramie County and $643.47 per month in the rest of the state.
High health-care costs have a negative impact on our state in many ways. First, they are a significant barrier for those working in economic development. It is hard to convince companies to come to Wyoming when they have to pay double or triple for health-care services.
Second, given that much of the Wyoming economy is based on commodities such as beef and coal, the high cost of our health care puts these products at a competitive disadvantage on both the US and global markets. Even our tourism industry is affected.
Don’t miss a WyoFile story — sign up for our free weekly newsletter
Third, the high cost of providing health benefits is preventing some employers from expanding, and forcing others to scale back or even close their doors. No one wants to put Wyoming doctors or hospitals out of business, but it often feels like those in the health-care industry — with a 50 year history of annual rate increases that are two and three (or more) times that of inflation — are trying to do just that to Wyoming’s businesses.

Finally, for individuals, the financial stress of unanticipated bills is the leading cause of personal bankruptcy. The human suffering involved is immeasurable.
Health-care costs are a problem. A big problem. The question is: what are we going to do about it? There is no silver bullet. No single change will fix all that ails health care. Addressing health-care costs in Wyoming will require a myriad of changes and extraordinary leadership from our hospital association, medical society, nursing association and every other stakeholder in this Byzantine business.
But let’s be honest; those in the health-care industry have no economic incentive to change the current system. Our fee-for-service payment methodology encourages those in the health-care delivery system to keep doing what they have been, which is what has gotten us into our current situation.
That is why the real leadership will have to come from employers who pay for health care.
Employers pay directly for their employees and their family members through the premiums they cover for their beneficiaries. Through taxes, they also contribute significantly to public programs such as Medicare and Medicaid. Those who pay the bills (either as an individual or a business) have a strong motivation to work for change. We see the cost of providing health benefits go up, year after year, at two to five times the price of any other input into our business or family budget.
We are at the breaking point.
Bills are up 67 percent, 7 times the increase in wages
Employers, be they private-sector or public-sector, can no longer absorb the cost increases, so they are passing them along to their employees in the form of higher deductibles and co-pays. Workers saw their share of the health-care bill increase 67 percent between 2010 and 2015. That is roughly seven times as much as wages grew during the same period.
Economists point out that our slow recovery from the Great Recession of 2008 is, in part, due to the dollars sucked out of every other economic sector by health care. The fact that health-care cost increases are outpacing wage growth also means that providers are having a hard time collecting on their bills, as patients simply can’t afford them. It is a vicious cycle.
Employers, concerned individuals and those in the health-care industry that understand the toxic nature of our current arrangement need to work together on systemic change. First, we need to understand that not all health care is the same. Several studies have shown huge variations in quality and price for the same test, procedure, or service — even in the same town.
Further, there appears to be no correlation between price and quality. In fact, some studies show that facilities with the best outcomes (highest quality) have the lowest costs. That’s because they get the diagnosis right faster, avoid unnecessary test and services, or don’t commit medical errors that add significant pain and suffering along with additional cost.
Those employers and patients who pay the bills need to demand transparency from the health-care industry — both in terms of price and quality. Once we are able to compare price and quality, we can empower our employees and their family members, as well as the general public, to be smart health-care consumers. We can search for ways to reward those who provide value (consistently good outcomes at competitive prices) as opposed to continuing our current system that rewards only volume.
We who pay the bills also need to look for, and reward, those who are innovative. In Cody, Dr. Allen Gee, a neurologist, has successfully helped many of his patients avoid painful and expensive back surgery. He researched other treatment options and now offers less invasive, less costly, but effective therapies. As payers, we need to find ways to reward Dr. Gee and others in Wyoming whose quest for value in health care is sincere.
Doing so requires us to find a different way to pay for health care. Our current fee-for-service system rewards those involved in amputating a diabetic’s foot, but not the providers who educate a diabetic about the disease, proper diet and self-care in order to avoid an amputation. We need to appropriately compensate those who prevent clogged arteries, not just those who perform bypass surgery.
However, once the doctor and patient determine surgery is necessary, we need to increase compensation to those who achieve better results at less cost. This may seem paradoxical, but we can pay more for necessary services if we can find ways to eliminate the estimated 30 percent of care that is clearly unnecessary.
Bundled payments reward for the entire “episode of care”
One method, called “bundled payments,” is being used across the country and early results show improvements in quality of care and reductions in overall cost. For example, think about how poorly your car would run if you bought the various engine components from different places with no thought or effort put into the overall design. Instead, you buy the complete package.
Currently patients and health-plan administrators get a myriad of disjointed and frequently incomprehensible bills all for the same episode of care. The fact is, the care provided is as uncoordinated as the billing. This is a huge problem.
Why can’t we set a single, all-inclusive price for all of the care required to treat a particular condition? By bundling the various services we can reward providers for working together, for doing a better job coordinating care and for being efficient. These bundles have proven to reshape the delivery system in four positive and important ways:
- Increased care coordination and integration: Under bundled payments, the various providers have a financial incentive to talk to each other and figure out the best course of treatment and the best method to execute that plan.
- Increased care innovation: As providers get rewarded for finding higher-quality and/or lower-cost methods of addressing medical issues, new and improved treatment will emerge. Care teams become common and the “team” includes the patient, physician(s) and other appropriate care providers.
- Accountability for cost and quality: By definition, bundled payments hold providers accountable to each other as well as the patient. Because bundled payments are risk-adjusted, providers are rewarded for taking on difficult cases. At the same time, they are penalized for over-treatment or inappropriate treatment. Patients, who typically lack medical training, are incapable of creating that accountability, but those on the care team with medical training have a financial incentive to ensure the entire cycle of care is done as well as it can be.
- Costs: Bundled payments motivate hospitals, physicians and other care providers to understand and analyze the actual costs of each step in the care process. This leads to more sophisticated cost/benefit analysis and continuous quality-improvement efforts.
For those who want to read further, a recent article in the Harvard Business Review provides a more in-depth look at bundled payments and the problems with fee-for-service. In Wyoming, no single payer is large enough to make any of these reforms come to pass. But working together, the employers across the state, public and private, large and small, can get educated and work together to effect change.
Employers need local political and health-care leaders to work with us. The process will not be simple, smooth or straightforward. We will encounter lots of obstacles. But the effort has to be made.
Anne Ladd is the CEO of the Wyoming Business Coalition on Health, an employer-driven nonprofit working to address health-care issues in and around Wyoming. WyBCH encourages all employers — public or private, large or small — to get involved in looking for solutions to the high cost of health care in Wyoming — Ed.
This was a wonderful refreshingly useful article that discussed the facts and reality of our nation’s healthcare crises. Ask a judge how many of their cases are really about the costs of health care. Our businesses all compete with other countries that have healthcare that doesn’t factor into their employees or the employers ability to compete.
Yes i have contacted many top officials in Wyoming on the findings of one hospital charging Medicaid around 500,000 dollars per child per year to house and medicate a child. I was able to save my child from this program…but it took a fight no parent should have to be put through…Just saying…this Institutionis am sure is hooked on Medicaid Money and needs an assessment..No one took me serious…they wil when I lawyer up…
I barely saved my childs life…she told me the doc told her he would put her on a feeding tube. It was during discharge did I learn she had been on amphetamine…and had some serious side affects because of it…
Healthcare Costs Cannot Be Controlled With a For-Profit System: A Suggestion for an Integrated Health Care System for Wyoming
Anne Ladd and Annemarie Albans have clearly described the negative drag Wyoming’s very high health care costs have on the overall economy of the state and to small businesses. Households, however, spend the most, accounting for 28% of all health care expenditures, making it a negative drag on consumer spending, as workers increasingly pay more for their health insurance, along with larger co-pays and deductibles. In real dollars, households contribute almost as much to health care as many governments spend on national health care for all of their citizens.
Health care expenditures, for the United States, have risen steadily from 5% GDP in 1960 to 17.5% in 2014. (During that same period European expenditures rose from about 5% to between 8 and 12%). Americans, however, are not three times healthier today than we were in 1960. In 1960 the top four causes of death were heart disease, cancer, stroke, and accidents, compared with heart disease, cancer, chronic respiratory disease, and accidents in 2015. Between 1960 and 2015, our life expectancy grew from 69.8 years to 79.3 years; during that period, other nations saw an improvement in their life expectancy but we fell behind, dropping from 16th to 31st place.
Despite multiple attempts to control health care costs, the ACA being the most recent, health care costs continue to rise. Ineluctably, they will continue to rise because in any for-profit business, profits are expected to increase quarterly. American is the only developed nation that has a for-profit health care system, which is why our health care costs are higher than any other nation. Economically, our system works like this: Pursuing economic growth, insurance companies raise prices and invent new ways to avoid unprofitable people and services; pharmaceuticals raise prices; providers raise prices; and doctors and hospitals duplicate each others’ services and find ways to avoid Medicaid and charity patients. In this system, the general public cannot protect itself. As a result, the numbers of uninsured and under-insured grow, as well as the public’s out-of-pocket costs.
The solution to continually rising costs is some kind of an integrated system. An integrated system means that providers and insurers work for the good of the whole, because they are part of the same system, e.g. Kaiser Permanente of Northern California or the Veterans Administration. An integrated system controls costs through global budgeting; equalizes access by including everyone; provides a uniform slate of benefits; assures the same level of reimbursement by pooling Medicare, Medicaid, and commercial insurance; and pays for value not volume by aligning incentives to control costs. In other words, physicians are not penalized for treating Medicaid patients, and all patients have access to all providers. Since all citizens are guaranteed a uniform slate of defined benefits, employers are freed from their annual hassle of shopping for health insurance due to insurance companies regularly changing their benefit packages, rules, and prices, and providers are freed from a massively wasteful billing nightmare.
Wyoming could develop, in stages, its own integrated health care system—much like North Dakota has its own state-owned bank. Eventually, each Wyomingite would have the same insurance card, the same benefits, and the same access, and providers would be freed from the costs of dealing with multiple insurers. The system could be funded with a combination of existing federal and state dollars, and progressive payroll tax, freeing businesses from the costs of administering health insurance for their employees and eliminating business free-riders. Eventually, all would be supported by a state-wide IT system that integrates doctors’ offices, hospitals, labs, pharmacies, and other services, and provides a single database for analytical purposes.
Some of the externalities associated with an integrated system include freeing employers from the medical costs of workers compensation, freeing the public from the medical costs of car insurance, reducing medical fraud, reducing medical malpractice lawsuits, and eliminating personal bankruptcies due to medical bills.
Despite the benefits, there are many challenges to creating an integrated system, including a waiver from federal law. The biggest challenge, perhaps, is the popular “health care is a consumer good” mindset, i.e. health care is a commodity, like a toaster or a truck, for those who can afford it. If we are to control costs, we need a new mindset, that health care is a “social good,” an essential safeguard of human life and dignity, available to everyone from cradle to grave.
While all stakeholders need to be involved, it is my impression that health care reform needs to be driven by the State for a number of reasons. The state is too small to buffer the cost-shifting that is bound to happen with four competing health care financing systems: Medicaid, Medicare, commercial, and health exchange insurances. The State has the purchasing power and the intellectual and economic resources necessary to support state-wide change. Moreover, it is the only entity large enough to assume the function, or create the entity that functions as the integrator, to coordinate services, and overcome multiple, competing self-interests.
Pete; you might want to write these lady’s name down.
We also might look at a very strong, analytical report by Atul Gawande ( http://www.newyorker.com/magazine/2009/06/01/the-cost-conundrum ) that went unnoticed in Wyoming and Casper in particular. He shows one of the drivers in the increasing cost of healthcare to be doctor-owned, for profit hospitals…