
Wyoming lawmakers are considering adding more regulations to an obscure yet powerful link in the pharmaceutical drug supply chain — pharmacy benefit managers. PBMs work behind-the-scenes as middlemen between insurance plans, drug manufacturers and pharmacies. Public scrutiny has led many states to pass legislation to better regulate PBMs. That includes Wyoming, which has added four PBM measures to its statutes since 2016.
Now, the Legislature is considering adding several more regulations to the books with House Bill 36 – Pharmacy benefit managers act enhancements. The bill has sparked much ado among lawmakers and stakeholders about how exactly PBMs work and who they are costing or saving money.
What’s a PBM?
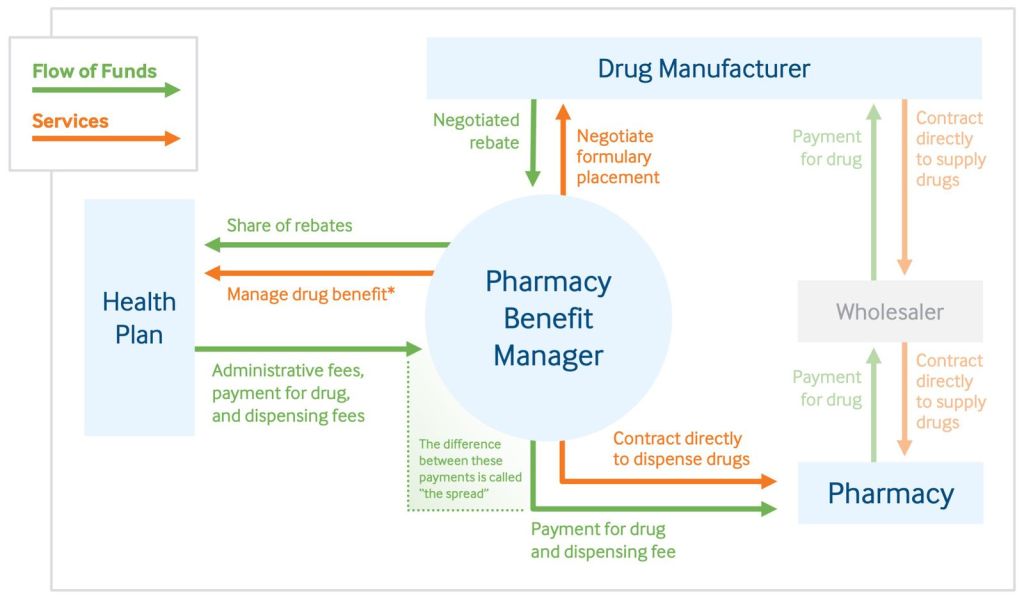
PBMs are multi-million dollar companies that manage prescription drug benefits on behalf of health insurers or large employers. They negotiate discounts, rebates and reimbursements, and purport to provide the sole source of downward pressure on the rising cost of drugs. They can also make money by pocketing some of the cash saved through those negotiations.
That’s where some parties, including many independent pharmacists in Wyoming, take issue. Last spring, more than 20 of them requested the Joint Labor, Health and Social Services Committee study PBM regulation in the last interim. The concerned pharmacists say such companies harm their businesses by not properly reimbursing them, and asked the committee to create legislation mimicking regulations passed by Arkansas.
House Bill 36 is that bill.
Cheyenne pharmacist Melinda Carroll spoke in favor of the bill during a House Labor, Health and Social Services Committee meeting Wednesday. The bill will make needed changes to the reimbursement process, she said.
PBMs reimburse pharmacies for the cost of drugs covered by insurer prescription drug plans. The health insurer, in turn, reimburses the PBM. Currently in Wyoming, PBMs have the ability to reimburse pharmacies at a lower cost than what the pharmacy paid to purchase the drug from a wholesaler. House Bill 36 would put restrictions on that practice.
These reimbursement discrepancies can be appealed by pharmacies, but the process lacks transparency. Part of the bill would establish a reporting requirement of PBMs to keep track of these appeals and provide that information to the state’s insurance commissioner each quarter.
“When they underpay us, we appeal to the very person that has already decided that they want to underpay us, so those appeals will be more public [under the bill],” Carroll said.
Pharmacists in favor of the bill argue that the current reimbursement process is hurting their bottom line and putting some in danger of going out of business.

Fiscal cost
The bill may save dollars for independent pharmacists, but concerns also exist about what it will cost the state. It’s estimated to cost the state Employees’ Group Insurance an additional $7 million annually. A lot of that has to do with a dispensing fee for prescriptions that would go into effect under the bill.
Bill sponsor Sen. Troy McKeown (R-Gillette) countered those concerns, implying the cost is worth it to help independent pharmacists.
“Are we willing to risk independence to save money for the state?” McKeown asked during Wednesday’s meeting.
But detractors of the bill say the fate of independent pharmacies is a matter of consumer choice. That included Johnson County Commission Chairman Bill Novotny, who spoke on behalf of the Wyoming County Commissioners Association. He told the committee the bill would cost counties up to an additional $20,000 a year.
The committee voted 3-2 in favor of the bill, with Sens. Fred Baldwin (R-Kemmerer) and Dan Furphy (R-Laramie) in opposition. Next week, the Senate Appropriations Committee will debate the bill and decide whether it’s worth the cost to the state.
You have a billion dollar industry that totally controls what you get paid, when you get paid, and don’t want to pay you. They can make up any type of rules then audit those rules that they know are in some cases impossible to follow on a daily basis. There is no checks and balances, no regulation they answer to no one. Yet the argument is if they pay us above our cost the price of health care will go up. Everything would go down if we all pay for a service below cost. As long as the pharmacies and let’s just throw in the doctors, the hospitals, the cost of groceries everything we deal with day to day, if you can get that entity to provide that service under their breakeven point everything costs less until that entity is no longer here. Pharmacies have no control of the cost of their product and then they are told what they have to sell that product for take or leave it. Let’s say the rancher buys a calf for $600.00 and he knows he has to sell it for $800.00 to break even due to his overhead (feed, fuel, equipment, labor, fencing , weed spraying, etc.) and you can only buy that calf from a couple of places . Then the buyer pays you $550.00, because on that particular breed that is all they pay, then they audit you and due to a blurry brand they fine you even more, and hold another $50.00 dollars called DIR fees for a year that they may or may not pay back. But now you have to buy another calf at $600.00 and this time you get $650.00 still under break even, and it goes on and on never quite reaching the break-even point. When you go to the optometrist you pay for their product the glasses and a professional fee for the exam. Pharmacies used to get paid for the medication and a filling fee, now there is no mark up for the product or a cost of living raise and the filling fee has dwindled to nothing. Even if they raise the filling fee they just pay less for the drug so even when you add the filling fee to the drug reimbursement you are still below cost. We need this bill to pass so we have someone to call and provide some type of checks and balances. The cost of the health care does not go up to the insurance companies or their clients it just makes the PBM’S give back the money they took from us and decrease’s their profits and makes them be more transparent and pay for the service we are providing for them.
First of all you have to understand the PBM’s have established a process that is basically like a carnival shell game, only they involve smoke and mirrors as more distraction. They will also make statements which are misleading such as “we pay your pharmacy” or “we negotiate discounts and rebates”.
I own a pharmacy and I will guarantee their contracts are take-it-or-leave-it and any rebates they negotiate with drug companies result in most of it going in their pockets and a token amount going to the plan sponsor. As far as payment being made to a pharmacy- there’s NO guarantee that the amount paid will cover what it cost the pharmacy to buy the medication and in fact at least half of our transactions result in the customers’s copay being the full amount the pharmacy gets paid. Pharmacies are seeing an alarming increase in prescriptions where the TOTAL price paid is less than $5- even for 90 day’s worth of a medication! We have even seen some as low as 30 CENT co-pays and the PBM pays nothing. That’s not the full travesty, though, because the employer plan can be asked to pay the PBM a price they allegedly paid the pharmacy. I have examples where my store was paid $2 by the PBM and the plan sponsor was billed $100, so the PBM made $98 on one bottle of cough syrup!!
Detractors of the bill say that the fate of independent pharmacies is a matter of consumer choice. That has been true of pharmacy ownership for years. But if PBM’s are allowed to continue to reimburse pharmacies at a rate below their actual cost to put the drug on their shelves, consumers will not have independent pharmacies as a choice. Box store and chain pharmacies suffer this loss also, but they have multimillions in additional inventory they sell to offset the loss in the pharmacy department. The independent does not have this luxury. Independent pharmacies provide a level of service you won’t ever find in a big chain operation. This bill is long overdue.